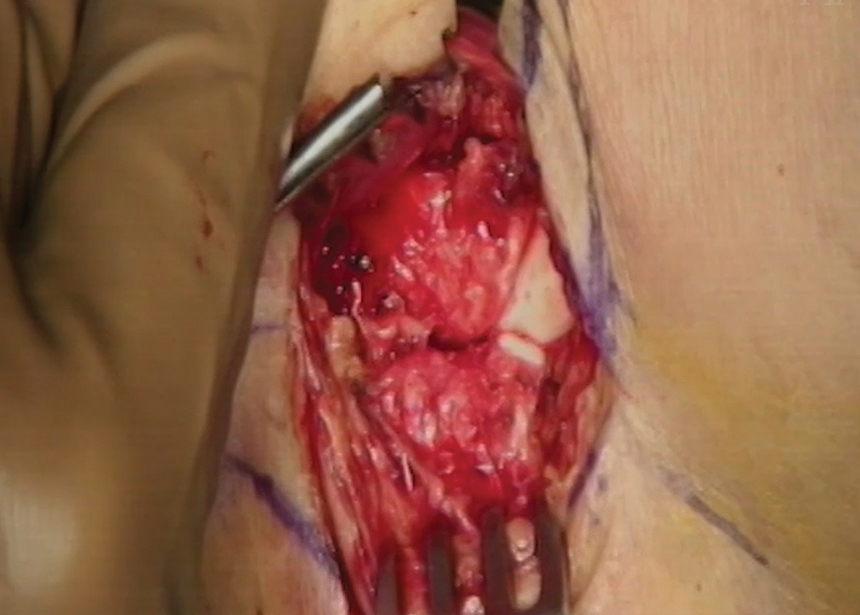
Fig 1. Mercedes sign showing syndesmotic reduction at the articular surface.
Author: Drew Krumm, MD;Karl Roberts, MD, FAAOS, FAOA
Category: Clinical;Foot & Ankle
Date: Sep 2023
Editor’s note: The following article is a review of a video available via the AAOS Orthopaedic Video Theater (OVT). AAOS Now will routinely review “OVT Plus” videos, which are vetted by topic experts and offer continuing medical education credits. For more information, visit aaos.org/OVT.
Regardless of specialty, many orthopaedic surgeons face the challenge of perfectly reducing the syndesmosis in the operative repair of ankle fractures. It is established in the orthopaedic literature that syndesmotic malreduction leads to poor outcomes. Reduction of the syndesmosis is commonly assessed via intraoperative fluoroscopic imaging, but open techniques allow for improved visualization.
An OVT video published in February 2021 by Paul Tornetta III, MD, PhD, FAAOS, demonstrates a mini-open reduction for an ankle fracture with associated syndesmotic injury. Direct visualization of the articular surface was used for assessment of syndesmotic reduction prior to fixation. This video has many useful pearls that can help orthopaedic surgeons obtain perfect reduction of syndesmosis.
Specifically, the relationship between the posterior fibula and posterior malleolus on a contralateral radiograph can be used as a template for alignment and reduction. However, concomitant posterior malleolar fracture can obscure this relationship, and in these cases, an open approach can be used to allow for direct visualization of syndesmotic reduction. This is represented by the Mercedes sign, which is made up of the anterolateral plafond, anteromedial fibula, and anterolateral talus (Fig. 1). Furthermore, careful placement of syndesmotic screws is paramount to prevent joint distraction or over-compression.
Operative technique
The video presents fixation of a right ankle fracture with lateral talar subluxation, widening of the syndesmosis at the incisura, and medial clear space widening. There is no overlap between the incisura and the medial aspect of the fibula on the mortise view. A small posterior malleolar fracture is seen on the lateral view. Contralateral radiographs demonstrate how the posterior fibula overlaps the posterior aspect of the tibiotalar joint.
A bolster is placed under the ankle joint, not the calcaneus, to avoid anterior subluxation. Under fluoroscopy, the corner of the anterolateral plafond and anteromedial fibula are marked. Stress views demonstrate widening of the medial clear space and syndesmosis. A 1.5 to 2.0 cm incision is made over the anterolateral ankle. Dissection is performed, being careful of the superficial peroneal nerve. After incising retinaculum, tissue is elevated from the anterolateral plafond to allow for visualization of the anterolateral joint surface and anteromedial fibula.
At this point, the syndesmosis and joint surface should be visualized. A Schnidt can be placed directly into the syndesmosis to show instability. The syndesmosis is manually reduced by adducting the talus. Once the syndesmosis is reduced at the articular surface, the Mercedes sign can be directly visualized between the anterolateral plafond, anteromedial fibula, and anterolateral talus. A Kirschner wire is placed obliquely from distal to proximal, outside the area of future syndesmotic screws, to provisionally hold the syndesmotic reduction. This is verified with a perfect lateral fluoroscopic radiograph. If a posterior malleolus fracture is present, the relationship between fibula and posterior malleolus can be obscured, necessitating open exposure to confirm reduction.
A position screw is then drilled across the syndesmosis just proximal to the tibiotalar joint. Counterpressure is placed on the medial malleolus as the screw is advanced as to not distract the joint. The screw is tightened by hand and not over-compressed. The K-wire is then removed, and reduction is reassessed with direct visualization. A second screw is placed 1.0 to 1.5 cm proximal to the first screw and is hand-tightened down to bone.
Intraoperative mortise view demonstrates good alignment and reconstruction of Shenton’s line, while the lateral view shows the position of the fibula just posterior to the edge of the articular aspect of the posterior malleolus. The deep synovial tissue and joint capsule are closed with 0-Vicryl in a vertical figure of eight fashion. The retinacular layer is then closed, ensuring no nerve branches are tied into the repair. The subcuticular layer is repaired, and staples are placed. Final radiographs are taken to assess mortise alignment, position of screws, Shenton’s line, and syndesmotic reduction.
Drew Krumm, MD, is a fifth-year orthopaedic surgery resident at Corewell Health/Michigan State University. He will be attending an orthopaedic trauma fellowship at University of Tennessee–Chattanooga in 2024.
Karl Roberts, MD, FAAOS, FAOA, is the program director for the Corewell Health/Michigan State University orthopaedic surgery residency program, chairman of the AAOS Evidence-based Quality and Value Committee, clinical advisor in orthopaedics and joint replacement for Corewell Health, and president of West Michigan Orthopaedics.
Title: Limited Open Syndesmotic Reduction with Intraoperative Radiographic Evaluation
Authors: Paul Tornetta III, MD, PhD, FAAOS
Published: Feb. 7, 2021
Time: 5:36
Tags: Featured, Foot and Ankle, Trauma Reconstruction, Radiograph, Reduction Techniques
Visit aaos.org/OVT to view this award-winning title and more than 1,200 other videos from across orthopaedic topics, institutions, practice management, and industry.